


1Leiden University, Faculty of Social and Behavioural Sciences, Institute of Psychology, Health, Medical and Neuropsychology Unit, 2Leiden Institute for Brain and Cognition, 4Department of Dermatology and 5Department of Psychiatry, Leiden University Medical Center, Leiden, The Netherlands, and 3Department of Experimental Clinical and Health Psychology, Ghent University, Ghent, Belgium
Placebo effects are positive outcomes that are not due to active treatment components, which may be elicited even when patients are aware of receiving an inert substance (open-label). This proof-of-principle study investigated for the first time whether open-label placebo effects on itch can be induced by verbal suggestions alone. Ninety-two healthy volunteers were randomized to experimental (open-label suggestions) or control (no suggestions) groups. Self-reported itch evoked by histamine iontophoresis was the primary study outcome. In addition, itch expectations, skin condition and affect were assessed. The experimental group expected lower itch than the control group, which was, in turn, related to less experienced itch in this group only, although no significantly different itch levels were reported between groups. The results illustrate a potential role for open-label placebo effects in itch, and suggest that further study of verbal suggestions through an extensive explanation of placebo effects might be promising for clinical practice.
Key words: placebo; expectancy; itch; verbal suggestions.
Accepted Oct 19, 2017; Epub ahead of print Oct 23, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Stefanie H. Meeuwis, Leiden University, Faculty of Social and Behavioural Sciences, Institute of Psychology, Health, Medical and Neuropsychology Unit, PO Box 9555, NL-2300 RB Leiden, The Netherlands. E-mail: s.h.meeuwis@fsw.leidenuniv.nl
Itch is the most common somatosensory symptom in skin conditions such as psoriasis and atopic dermatitis, and can cause significant impairment in patients (1). For example, itch has previously been associated with impaired quality of life, a reduction in social activities, reduced quality of sleep, concentration problems, and depression (2). Current treatments are often aimed at reducing the severity of the skin condition through pharmacological interventions with, for example, (topical) antihistamines or corticosteroids. However, these interventions have usually shown limited effects and are often accompanied by side-effects (3, 4). Over recent years, researchers have aimed to identify other factors involved in the experience of itch that might be used to improve treatment effectiveness (5). A promising factor influencing the experience of itch without requiring medication is the placebo effect (6–8).
Placebo effects are beneficial effects of pharmacologically inert treatment components (6, 8). A recent meta-analysis indicated that itch may be especially prone to such effects, and that up to 30% of improvement in itch may be attributed to the occurrence of placebo effects rather than pharmacological intervention (9). Experimental studies further demonstrate that placebo effects can be induced in itch by providing suggestions that a treatment is able to alleviate itch, or by suggesting that a test that generally provokes itch will elicit no itch (10, 11). In addition, there is evidence that the opposite instructions (e.g. suggesting that a treatment will sensitize a person to itch) can increase itch, a phenomenon known as the nocebo effect (10, 12–14). In addition to studies investigating the effects of verbal suggestions on self-report measures such as itch, a few studies have investigated whether verbal suggestions can influence physical skin conditions, for example wheal and flare size in response to histamine (11, 12, 14, 15). It has been demonstrated recently that negative outcome expectations, or nocebo, can result in a greater physical skin response, as demonstrated by larger flare size in response to histamine and wheal size in response to natrium chloride following negative verbal suggestions (14). Placebo (and nocebo) effects can be established by a patient’s belief in treatment effectiveness and outcomes (6, 8, 16–18). The main working mechanisms of placebo effects include associative learning processes, such as conditioning, and expectations, such as positive information regarding treatment outcomes provided by means of verbal suggestions (6, 8, 16, 18).
Most studies on placebo effects have used an experimental approach eliciting placebo effects by providing uncertainty or deception about the specific treatment provided (e.g. actual medicine or placebo). It is assumed that the benefits that patients experience from inert substances stem from the covert belief that a pharmacologically effective treatment is being given (19). This uncertainty or deceptive component complicates the potential utilization of placebo effects in clinical practice, considering that omission of treatment information and provision of deceptive information are unethical (18, 20). Studies have, however, indicated that a placebo treatment can still be effective when patients are aware of receiving an inert treatment (21–28). Most of these studies on open-label placebo treatment have reported medium-to-large effect sizes (21, 22, 25), comparable to the effect sizes found by studies in which patients were not informed about receiving an inert substance (closed-label placebo; (29)). A recent pilot study furthermore demonstrated that such an open-label placebo treatment may also be effective for symptoms of allergic rhinitis, including itch (28). Within this pilot study, symptom improvement by open-label placebo treatment was furthermore associated with higher subjective well-being (28).
It is not yet clear by which mechanisms open-label placebo effects may be elicited. Previous open-label studies have combined different components, namely the administration of an inert pill and a rationale concerning placebo effectiveness and its mechanisms (21–28). This complicates the understanding of which of these components contribute to open-label placebo effects, or the extent to which they contribute. It is not yet known whether providing a positive rationale (e.g. verbal suggestions) exclusively might be sufficient to induce open-label placebo effects by changing expectations regarding itch and affecting the response to an itch stimulus. If proven possible, this would facilitate clinical applications; for example, by optimizing existing treatment methods for chronic itch by improving doctor–patient communication.
The aim of the current proof-of-principle study was to investigate for the first time in an open-label design whether positive verbal suggestions about itch in response to an itch-provoking test without combining it with an inert treatment can induce positive outcome expectancies and reduce self-reported itch in response to a short-term itch-provoking histamine test. Physical and self-reported skin condition and positive and negative affect were secondary outcomes. In addition, the specific role of expectations in the effects of open-label verbal suggestions on itch was examined. It was expected that open-label positive verbal suggestions about itch would reduce the level of itch that participants expected to experience during the histamine test as well as the mean level of itch experienced during the test, compared with a control condition that received no verbal suggestions. In addition, it was expected that open-label positive verbal suggestions compared with the control group would reduce the severity of the participants’ skin condition, and that verbal suggestions would diminish changes in positive and negative affect as a consequence of itch induction by histamine iontophoresis.
The study was approved by the Medical Ethical Committee at the Leiden University Medical Center, The Netherlands (protocol number NL54570.058.15) and performed in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Healthy male and female volunteers were recruited primarily through advertisements and flyers at various sites of Leiden University, The Netherlands, and through online media. Participants were included if they were between 18 and 35 years old and had a sufficient understanding of written and spoken Dutch. Exclusion criteria consisted of severe somatic or psychological morbidity (e.g. heart and lung diseases, histamine intolerance, or the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) psychiatric diagnoses) that might interfere with the study protocol, current chronic itch or pain complaints, current medication use (analgesics, anti-inflammatory drugs, antihistamines, or antibiotics), or pregnancy. In order to prevent potential influences on the response to the itch stimulus, participants were asked to refrain from the consumption of food, caffeine, and smoking 2 h prior to the laboratory session. In addition, they were asked to avoid heavy exercise 12 h, and alcohol and drugs 24 h prior to the session. This was verified at the beginning of the laboratory session, including a brief check of participant eligibility.
A between-subjects experimental randomized controlled trial design was used. Subjects considered eligible to participate in the study were invited to a 1-h laboratory session and randomized to either the experimental (i.e. open-label positive verbal suggestions) group or the control (no verbal suggestions) group. The randomization sequence was acquired through the use of an online random number generator (www.random.org, Dublin, Ireland). The laboratory session was conducted by 2 experimenters; only one of whom was aware of group allocation and provided the verbal suggestions. Participants and the experimenter who conducted the outcome assessments were unaware of group allocation during the laboratory session.
Histamine iontophoresis. Histamine was applied to the skin through transdermal iontophoresis (Chattanooga Group, Hixson, TN, USA). This method has been used previously to experimentally induce itch in healthy volunteers (10, 30, 31). A 0.3% diphosphate histamine solution was prepared in distilled water with propylene glycol and hypromellose 4000 mPa. An electrode (Iogel, Iomed, DJO Global, Hannover, Germany) was prepared that contained 2.5 ml of the histamine solution. The electrode had an active area of 11.7 cm2 and was placed on the volar side of the non-dominant forearm, and the reference electrode was placed on the volar surface of the upper arm. Current level was set at 0.4 mA. Histamine iontophoresis was applied for 2.5 min, after which the electrodes were removed and a follow-up period of 4 min was started.
Verbal suggestions. Participants were informed prior to the session that the study aimed to investigate individual differences in the experience of itch. Upon arrival at the laboratory session, the following general instructions were given to all participants: “During the test, histamine will be applied on your skin by means of a small electrical current. This elicits a response that is similar to a mosquito bite. Your skin may become red and may swell up.”
In the experimental group exclusively, participants were given the following verbal suggestion, followed by an open-label instruction: “Previous research indicates that the test elicits little or no itch in most healthy people, meaning in 95% of cases. We would also like to give you some extra information. From research we know that expectations play a large role in how itch is experienced, for example through giving information about what to expect from a test such as this one. I just told you that the test that you are about to do elicits little or no itch in most healthy people. From research we know that this suggestion will really cause people to experience little itch, even when they are aware of receiving this suggestion. Thus, the suggestion alone that the test causes little or no itch will already cause you to experience little itch.”
Process measure: expectations about itch. Participants were asked to indicate on the computer the level of itch they expected to experience, using a numerical rating scale (NRS) ranging from 0 (“no itch at all”) to 10 (“worst itch ever experienced”). Expected itch was assessed at 2 time-points during the laboratory session: once during baseline assessments and once after the verbal suggestions but before the histamine iontophoresis.
Primary outcome measure: self-reported itch. The level of experienced itch during histamine iontophoresis was assessed verbally every 30 s during iontophoresis and during a 4-min follow-up period, using the same NRS as described in the previous paragraph. Directly following histamine iontophoresis, the mean experienced itch during iontophoresis was assessed verbally using the same NRS. As part of a series of online questionnaires that assessed baseline measures (see Procedure), the level of itch experienced prior to iontophoresis was measured graphically by dragging a slider over a bar slide using the same NRS, with a 2-decimal score depicted next to the bar slide.
Secondary outcome measure: physical skin condition. Wheal size and flare size in response to histamine iontophoresis were traced on a 1 cm2 gridded, transparent sheet following histamine application using a 0.4-mm black permanent marker (Staedtler, Germany). Scans of the sheets were then uploaded and analysed using ImageJ (32). Images were calibrated to the 1 cm2 grid in ImageJ, after which wheal and flare area were estimated in cm2 through tracking the outer edges of the drawn wheal and flare areas. In addition, skin temperature was assessed following histamine iontophoresis on the application site on the arm using a hand-held infrared digital thermometer (accuracy ±2.0°C, resolution 0.1°C, BaseTech, Conrad Electronic Benelux B.V., Hirschau, Germany). The thermometer was held vertically approximately 1 cm above the area. To control for individual differences in skin temperature, a second measurement was taken of a similar skin area of the contralateral arm and used as a covariate in the analysis.
Secondary outcome measure: self-reported skin condition. The Sensitive Scale-10 (SS-10) was used to assess self-reported skin condition (33). This scale assesses the severity of skin sensitivity over the past 3 days through evaluation of 9 skin condition items (e.g. burning, tautness, itch, and redness of the skin) on a 0 (“zero intensity”) to 10 (“intolerable intensity”) scale. In addition, the scale assesses skin irritation on a visual analogue scale (VAS), ranging from 0 to 10 (33). The SS-10 total score was calculated by summing all items, with a higher score indicating more intense skin sensations (range 0–100). Upon arrival in the laboratory, participants completed the SS-10 for a baseline measurement. A slightly adjusted version of the SS-10 was used to assess self-reported skin condition following histamine iontophoresis, with participants having to indicate the symptoms experienced during histamine iontophoresis rather than symptoms experienced during the past 3 days. In the current study, Cronbach’s alpha was 0.83 for baseline SS-10 and 0.89 for the adjusted post-test SS-10.
Secondary outcome measure: positive and negative affect. The Positive and Negative Affect Schedule (PANAS) was used to assess positive (PA) and negative affect (NA; (34)). In this 20-item questionnaire, participants indicated the extent to which they experience specific emotions (e.g. interested, excited, or nervous) at that moment on a 1 (“very slightly or not at all”) to 5 (“extremely”) scale. PA total score was calculated by summing the 10 positive items of the scale and NA total score by summing the 10 negative items (total score range 10–50, with higher scores indicating higher PA or NA). Baseline affect was measured upon arrival in the laboratory (baseline PA and NA) and following histamine iontophoresis (post-test PA and NA). Cronbach’s alpha was 0.83 for baseline PA and 0.79 for post-test PA. For NA, Cronbach’s alpha was 0.82 and 0.91, respectively. To examine group differences in the changes over time in positive and negative affect in response to the histamine iontophoresis, PA and NA change scores were calculated for each scale by subtracting baseline scores from post-test scores. For both positive and negative affect change scores, positive scores indicated an increase in that particular affect.
Prior to being invited to a laboratory session, participants were provided with written information about the study. Participants subsequently completed a series of online questionnaires assessing the screening criteria and several personality characteristics, which are not described here since they are unrelated to the aim of the current study. Prior to this, participants provided written informed consent for the online questionnaires. At the start of the laboratory session, the study procedures were explained to all participants and written informed consent for the entire study was provided, following which participants were given instructions regarding the histamine test by the first experimenter. Next, baseline measurements were taken of itch, self-reported skin condition, positive and negative affect, and itch expectations before verbal suggestions. Positive expectations were then induced through open-label verbal suggestions in the experimental group. Participants then again indicated the level of itch they expected to experience. In the meantime, the first experimenter left the room and was replaced with the second experimenter. Histamine iontophoresis was then conducted by this second experimenter. During histamine iontophoresis as well as during the 4-min follow-up period, the level of itch participants experienced was assessed verbally on the NRS every 30 s. Directly following iontophoresis, mean experienced itch during iontophoresis was assessed, again using the same NRS. Subsequently, measurements of physical skin condition (e.g. wheal, flare) were taken and post-test questionnaires SS-10 and PANAS were administered. The second experimenter was then replaced by the first experimenter and participants were debriefed about group allocation and the true purpose of the study.
A power calculation for an analysis of covariance (ANCOVA) using G*Power 3.1 (35) indicated that a total of 92 participants was needed to achieve a power of β=0.80 at a 2-sided significance level of α=0.05 to detect a Cohen’s d effect size of at least 0.30 on the primary outcome measure of mean itch. Analyses were performed using SPSS 21.0 for Windows (IBM SPSS Inc., Chicago, IL, USA). Variables were checked for normal distribution. In order to achieve normal distributions, square root transformations were applied for baseline itch and self-reported skin condition, as well as the physical skin condition parameters wheal size and flare response, and a log10 transformation was applied to baseline skin temperature. For PANAS negative affect change scores, transformations failed to achieve a normal distribution; therefore, a non-parametric Kruskal–Wallis test was used to examine group differences on this outcome measure. χ2 tests and general linear model (GLM) ANOVAs were used to detect differences between groups on demographic factors and baseline measurements of itch, self-reported skin condition (SS-10), and positive and negative affect. The primary outcome measure of mean experienced itch, as rated by participants following histamine iontophoresis (mean ± standard deviation (SD) 3.3 ± 1.6) was correlated very highly with the mean score of itch ratings during the histamine iontophoresis (mean ± SD 2.9 ± 1.4; r = 0.93, p < 0.001), supporting the reliability of the itch measure used. To examine whether the groups differed on the process measure of itch expectation (post-verbal suggestions) and on the primary outcome of mean itch experienced during the histamine test, 2 GLM ANCOVAs were conducted, with baseline expectations and baseline itch level included as covariates in the analyses, respectively. Similar ANCOVAs were conducted for the secondary outcome measures of the SS-10 and skin temperature. For wheal and flare size in response to histamine iontophoresis, as well as for PANAS positive affect change scores, GLM ANOVAs were performed. As an effect size measure, Cohen’s d was calculated for analyses on the primary and secondary outcome parameters, with d = 0.2, 0.5 and 0.8 being interpreted as a small, medium and large effects, respectively (36). In order to explore whether itch expectation after the verbal suggestions was related to the level of mean experienced itch during histamine iontophoresis, and whether this relationship differed between groups, separate effects, as well as an interaction effect of post-verbal suggestions itch expectation and group, were examined in a multiple regression analysis, with baseline itch and pre-verbal suggestions itch expectation as covariates. Post-verbal suggestions itch expectation was centred prior to the analysis. All analyses were conducted 2-sided with a significance level of α < 0.05.
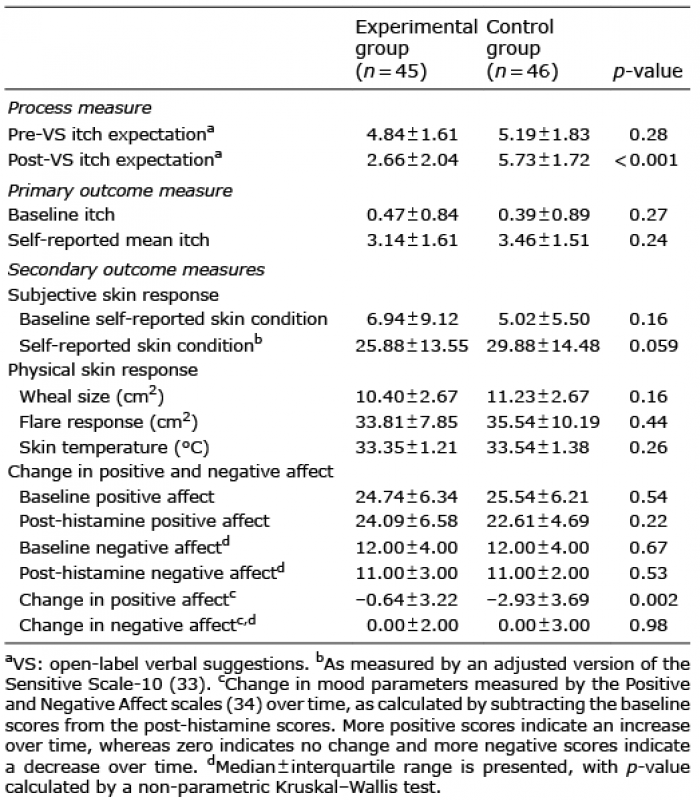
A total of 139 potential participants expressed interest in the study, of whom 24 were excluded due to medical morbidity (e.g. migraine, asthma, presence of a skin disorder) and 9 due to psychological morbidity (e.g. depression, anxiety). In addition, 14 persons refrained from participation for other reasons (e.g. no response after first postal contact). In total, the sample consisted of 92 healthy male (n = 17) and female (n = 75) participants between 18 and 26 years of age (mean ± SD 21.3 ± 1.9 years). Participants were of Dutch (98%), Dutch–Turkish (1%), or German (1%) nationality. Of all participants, 41% had a partner, of whom 7% were living with a partner or were married. Of the female participants, 69% used oral contraceptives. Randomization resulted in a total of 46 participants in the experimental group and 46 participants in the control group. Data for one participant in the experimental group were excluded from analysis, due to technical issues during histamine iontophoresis. χ2 tests and ANCOVAs revealed no differences between groups with regard to age, sex, education, or nationality (all p-values ≥ 0.19). Table I displays the means ± SD for the baseline measurements, and the primary and secondary study outcomes for the 2 groups.
Table I. Means ± standard deviations for baseline and outcome measures of study parameters per group
As shown in Fig. 1, in the experimental group significantly lower itch expectations were reported following verbal suggestions (mean ± SD 2.66 ± 2.04) than in the control group (mean ± SD 5.73 ± 1.51). A statistically significant large-sized effect of verbal suggestions on post-verbal suggestions itch expectation, controlled for pre-verbal suggestions itch expectation, was demonstrated in the ANCOVA; F(1, 89)=59.57, p < 0.001, Cohen’s d = 1.62.
Fig. 1. Mean numerical rating scale scores for the experimental (open-label positive verbal suggestions; n = 45) and control (no suggestions; n = 46) group for the process measure and primary study outcome measure. (A) Expected itch on the histamine iontophoresis test before and after instructions. (B) Mean itch in response to histamine iontophoresis. Error bars represent standard error of the mean. ***p < 0.001.
No statistically significant difference between groups in mean self-reported itch in response to histamine iontophoresis, controlled for baseline itch, was found in the ANCOVA; F(1, 90)=1.40, p = 0.24, Cohen’s d = 0.21.
Multiple regression analysis to test for interaction effects between post-verbal suggestions itch expectation and group on self-reported mean itch during histamine iontophoresis did not show significant main effects for group (β = 0.06, p = 0.69) or post-verbal suggestions expected itch (β = 0.36, p = 0.10). As expected, baseline itch and pre-verbal suggestions expected itch were not predictive of self-reported mean itch during histamine iontophoresis (p ≥ 0.36). However, a statistically significant interaction effect for group × post-verbal suggestions itch expectation was found (p = 0.04), indicating that in the experimental group only, lower expected itch was associated with lower self-reported mean itch during the histamine iontophoresis, whereas no association between expected and experienced itch was found in the control group (full model: R2=0.11, F(5,89)=2.04, p = 0.08; see also Fig. 2).
Fig. 2. Scatter plot of the interaction effect between expected itch following verbal suggestions, controlled for pre-verbal suggestions expected itch, and group (experimental, n = 45 and control, n = 46) on self-reported mean itch during histamine iontophoresis controlled for baseline itch.
Self-reported skin condition (SS10) scores following histamine iontophoresis were marginally significantly lower, indicating better self-reported skin condition, in the experimental group (25.88 ± 13.55) than in the control group (29.88 ± 14.48; F(1, 90)=3.67, p = 0.059, Cohen’s d = 0.29). No statistically significant group differences were found for the physical parameters wheal and flare size, and skin temperature in response to histamine iontophoresis (p ≥ 0.14).
A statistically significant and medium-sized effect of verbal suggestions on PA change scores was demonstrated compared with the control group; F(1, 90)=9.93, p = 0.002, Cohen’s d = 0.66. Participants in the control group showed a stronger decline in positive affect from before to after the histamine iontophoresis (mean ± SD PA change score –2.93 ± 3.69, range –15 to 5), whereas participants in the experimental group remained more stable over time (mean ± SD PA change score –0.64 ± 3.22, range –8 to 8). The Kruskal–Wallis test revealed no statistically significant difference in NA change scores between the experimental and control groups (p = 0.98).
This proof-of principle study investigated for the first time whether open-label positive verbal suggestions alone can induce outcome expectations and reduce the level of itch experienced during histamine iontophoresis. It was demonstrated that the open-label positive verbal suggestions were successful in reducing the level of itch participants expected to experience during histamine iontophoresis, but not in reducing itch experienced in response to the histamine test. The relevance of expectations was demonstrated further by showing that a decrease in expected itch in response to verbal suggestions was significantly associated with lower experienced itch in response to the histamine test in the experimental group, but not in the control group. Moreover, a tendency was found for patients to rate the severity of the self-reported skin condition as lower following open-label suggestions, compared with the control group, but no effects on physical skin condition were found. Furthermore, a significantly smaller decrease in positive, but not negative, affect was found in response to the histamine test in the verbal suggestions group, compared with the control group.
These findings, that open-label positive verbal suggestions did not affect actual experienced level of itch, are not in line with the findings of previous studies on open-label placebo in, for example, allergic rhinitis, low-back pain and irritable bowel syndrome (21–26, 28). This may be due to the current study using verbal suggestions exclusively without an inert treatment. In previous studies, open-label placebo effects have been induced by asking participants to ingest pharmacologically inert pills combined with providing a suggestive positive rationale to participants, in which it was explained how placebo effects induce symptom improvement and in which the effectiveness of placebo treatment was emphasized (21, 22, 28). It is possible that the mere act of taking medicine could have elicited stronger placebo effects. Influential conditioning theories of placebo effects state that the placebo effect is a conditioned response that is a result of previously learned associations (16). As pointed out previously by Carvalho et al. (21), the rituals surrounding administration of medication may have activated previously learned associations between symptom alleviation and capsule or pill ingestion. Considering that all previous open-label studies have been conducted in patient populations in which medication administration is common, it seems likely that these effects were further strengthened by associative learning pathways and heightened relevance of symptom improvement for patients in these studies. The current study, on the contrary, sought to examine the ability to elicit placebo effects by provision of positive verbal suggestions without coupling with an inert substance in healthy participants. Investigating these effects not only provides information regarding the mechanisms of open-label placebo, but if proven possible would also allow for easier implementation in clinical practice, for example by optimizing the information provided to patients in existing treatment in order to maximize placebo effects. The placebo effects induced in the current study may have had some impact, as evidenced by the successful expectation induction, which was in turn related to lower itch level, but speculatively may not have been strong enough to significantly alter the way in which itch was actually perceived in response to the itch stimulus.
Next to effects on itch expectancy, there was also a tendency for participants in the experimental group to indicate better self-reported skin condition following the histamine test than controls. That positive affect in the open-label suggestions group also decreased significantly less than in the control group upon itch induction also indicates that some effects may have occurred. This may be compared with the previous finding that improvement in allergic rhinitis by open-label placebo treatment is related to higher wellbeing (28). However, no effects of open-label positive verbal suggestions on physical skin condition (i.e. wheal and flare size, skin temperature) were found, which is in line with previous findings for closed-label placebo effects on physical skin responses (11, 15), but not with findings for closed-label nocebo effects on physical skin response (14). Although indications were found that the verbal suggestions may have mostly influenced subjective measures, they were potentially not strong enough to significantly alter the symptom and physical outcomes between groups.
In this study, a potential predictive role of a change in itch expectations due to open-label verbal suggestions was observed for the resultant itch level that was reported in response to the histamine test, showing that a larger decrease in itch expectations was associated with lower experienced itch. This is in accordance with the idea that placebo effects can impact symptoms by means of changing people’s expectations and is in line with the provided rationale explaining that expectations can alter the way in which itch can be perceived. Whereas in closed-label placebo studies the expectation that a certain treatment or medicine results in symptom improvement is attributed to the provision of uncertainty or deceptive information by the doctor or experimenter (27, 37), in open-label studies this might be attributed to the provision of a rationale on how placebo effects could instead lead to beneficial treatment outcomes. For both, the actual expectation of symptom improvement of the patient is suggested to be present and to have an impact. Previous studies, however, have always combined open-label placebo pill administration with the rationale that explained that “the placebo effect can be powerful” and that “the body may respond automatically to placebo treatment” (21, 22, 28). Furthermore, as in most of these trials, open-label placebo treatment was given along with treatment as usual (21, 22, 28) and the effects that patients might experience were not specified, placebo effects may have been enlarged by simultaneously occurring pharmacologically-induced reduction in symptoms. As such, it is difficult to determine the exact underlying cause of placebo effects in these studies. Demonstrating that placebo effects could be exclusively due to a positive rationale, on the other hand, would facilitate easier implementation in clinical practice, as no additional inert pills would need to be given. Instead, a positive framework for patients in which placebo mechanisms are illustrated could then potentially suffice to strengthen existing treatment methods for itch.
Some strengths and limitations of this study need to be taken into account. This is the first study to examine the ability of positive verbal suggestions to induce placebo effects in itch in an experimental, open-label design without combining it with an inert treatment. The relatively large sample size and use of a homogenous participant group allowed for a robust indication of effect sizes. Assessment of outcome variables was conducted by an experimenter who was blinded to group allocation in order to minimalize reporting bias. However, as in all research in which placebo effects are induced by verbal suggestions, reporting bias cannot be ruled out, as participants may still have adjusted their answers due to the explicit instructions on expectations. Fourthly, participants underwent histamine iontophoresis only once and most were unfamiliar with histamine iontophoresis. Prior to the test, participants were told that the response to histamine iontophoresis could feel like a mosquito bite. However, since the participants did not know exactly what to expect during the test, this lack of a reference frame for itch may have complicated changing these expectations and, consequently, the induction of placebo effects. Future studies could examine whether providing a more familiar stimulus, for example by providing a baseline test prior to placebo induction, would lead to clearer expectation effects (13). Finally, while in the open-label verbal suggestions a distinction was made between the suggestion (i.e. “research indicates that the tests elicits little to no itch in most healthy people, meaning in 95% of cases”) and the open-label rationale, both were given to one group only. As such, we cannot distinguish between effects of the suggestion itself and the open-label rationale that followed. For future research, it may also be useful to compare open-label with closed-label placebo induction, in order to better distinguish between open- and closed-label placebo effects in itch.
In conclusion, this proof-of-principle study indicates for the first time that open-label positive verbal suggestions were able to reduce itch expectations prior to a histamine test. Also, open-label suggestions were associated with a smaller impact on positive affect and indications were found for a more positive self-perceived, but not physical, skin condition in response to the validated histamine test. However, the suggestions did not significantly impact actual itch levels between groups, although within the experimental group an association was found between expected and experienced itch after verbal suggestions. Future research should aim to strengthen the open-label verbal suggestions, for example by providing a more explicit explanation of placebo mechanisms and effectiveness, in order to investigate whether open-label placebo effects can be induced in itch without the need to administer a substance.
This study was funded by a European Research Council Consolidator Grant 2013 (ID: ERC-2013-CoG-617700_EXPECT HEAL-TH, granted to AE). The funders had no role in study design, data collection or analysis, decision to publish, or in writing this manuscript. Jan De Houwer is supported by Ghent University Methusalem Grant BOF16/MET_V/002.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize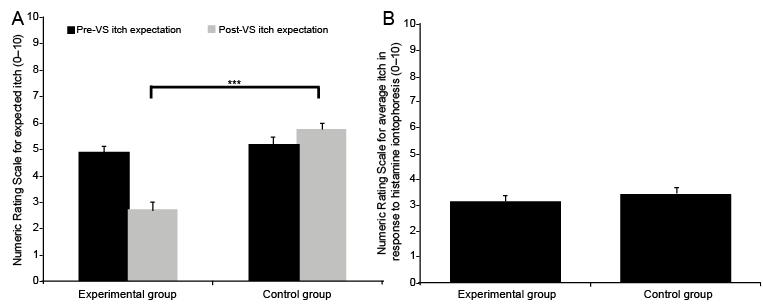 Click to show fullsize
Click to show fullsize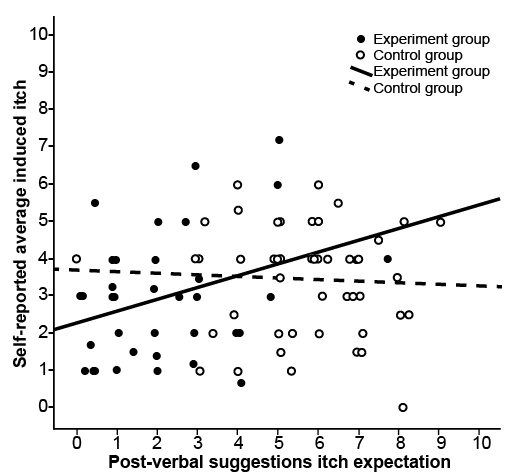 Click to show fullsize
Click to show fullsize